Having the optimal motion and mobility at each joint allows the body to utilize the architecture of the joint and the soft-tissue structures to the best of their ability.
Research has linked limited dorsiflexion to injuries in the lower leg, such as plantar fasciitis, shin splints, stress fractures, ankle sprains and Achilles tendinitis. Two-legged squatting with limited dorsiflexion increases knee valgus, decreases quadriceps activity and increases soleus activity. In addition, limited dorsiflexion in jump landing has been tied to increased ground reaction forces, reduced knee flexion and increased knee valgus—all of which increase the risk of anterior cruciate ligatment (ACL) injury.
Improving ankle mobility requires much more than myofascial release of the calves and stretching the calves with the ankle in dorsiflexion in the sagittal plane.
|
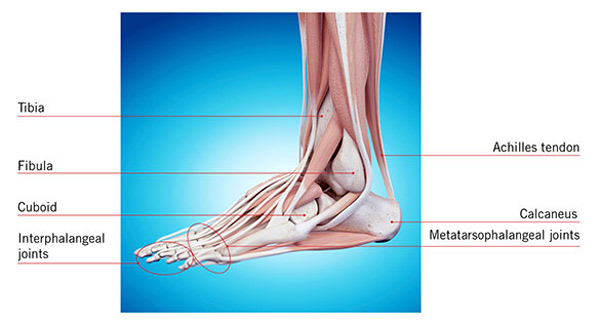
If we consider the bony geometry of the foot and ankle and the continuity of the myofascial tissue at the back of the gastrocnemius and soleus to the metatarsal heads, and cranially with the relationship to the hamstrings, we can see many overlooked opportunities to improve ankle mobility. The foot and ankle consist of a combined 26 bones that make up 33 joints. By involving the complementary motions of these joints and the associated soft tissues that act on them, we can identify an abundance of ways to develop mobility strategies.
Incorporate the following exercises for enhanced ankle mobility:

- Self-myofascial Release Exercise: Using a small ball or series of small balls of varying sizes and densities. Move from the bottom of the foot to the posterior lower leg using a roller. Use a tennis ball or similarly sized ball to target areas of the lower leg with more specificity. For example, you can target the tissue between the lateral gastrocnemius/soleus and the peroneals. Work your way up to the hamstrings to include all three muscles by rotating the thigh slightly to address the medial and lateral aspects of this muscle group.
- Self-mobilization of the Ankle Joint: Using a flat piece of elastic band, anchor it behind the foot through the loop made in the tube. Place the tubing across the very bottom of the ankle and over the talus. Create tension on the band by moving farther away from the anchor. From there, bend the knee and drive it over the front of the foot into ankle dorsiflexion. As the tibia and fibula move forward over the talus, the tubing pulls the talus back and assists its glide into the mortise. This can be performed for multiple repetitions to assist the articulation of the joint and provide the bony clearance necessary for improved dorsiflexion.
- Dynamic Stretching: Position a stable object such as a 2- to 3-inch high half-foam roller about 2 feet from a wall. Place the hands on the wall at chest level for stability and place the forefoot of one foot on the object with the heel on the ground to create some initial pre-stretch. To maximize the benefits of the lengthening of all of the involved tissue, hold the toes in extension from the object elevating the forefoot. Keep the involved knee straight in a “soft” extension.
- Back Leg Raise: Holding on the position as in dynamic stretching, start with the uninvolved hip and knee flexed to 90 degrees. Reach back with the uninvolved leg and straighten as it passes the other leg. The torso simultaneously hinges forward at the hip, bringing the head and torso closer to the wall. This action of the torso coming forward should increase knee extension of the involved leg and progressively increase the stretch/tension from the calf up into the hamstring. Return to the starting position in a smooth, controlled motion and repeat. Perform this movement continuously for the recommended five to 10 repetitions.
- Side Rotation: The starting position is the same as in Back Leg Raise, with the hip and knee of the uninvolved leg flexed to 90 degrees. While maintaining the 90 degrees of hip flexion, bring that limb across the body. The femur of the involved leg rotates slightly in relation to the tibia below, causing the subtalar joint of the involved leg to invert and midtarsal joint to supinate. This creates an additional transverse axis in which the tissue is lengthened. The uninvolved leg is then brought back across the body and rotated farther from the start position into abduction. This motion creates subtalar joint eversion and midtarsal joint pronation. It also creates another transverse axis—opposite to the previous movement—as the tissue is elongated in a different direction.
Ankle and foot mobility are dynamic processes that are not limited to one direction. Therefore, an effective mobility strategy should address as much variability in tissue extensibility as possible. This can be accomplished by applying motion in relation to the multiple joint structures involved.
Reference:
Related Links
- Tips to Protect Your Joints While Practicing Yoga
- Top 10 Tips on Prevention of Sports Injury
- Yoga to Heal and Prevent Shin Splints
- Ankle Sprain
- Working the Hamstring
Disclaimer
The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.